“The best test for the prediction of the risk of atherosclerosis, is the demonstration of atherosclerosis” Ernest Schaeffer, Editor-in-Chief, Atherosclerosis
Dr Lawrence Dembo
Cardiologist
Former Head (2008-2021): Advanced Heart Failure and Cardiac Transplant Service of Western Australia
Director & Medical Imager: Envision Medical Imaging
The Coronary Calcium Score
The calcium score is the most powerful risk factor for future cardiovascular event
Why? Because, Calcium is direct, visible evidence of coronary artery disease whilst the standard risk factors are only risks of atherosclerosis. An elderly patient with a full house of risk factors and calcium score of zero has a very low risk. A young patient with no risk factors and a very high calcium score has an extremely high risk of future coronary artery disease.
Atheroma occurs with inflammatory changes in the wall of the coronary artery. Over time, some of the inflamed “soft” plaques heal. A byproduct of this chronic inflammation is calcium deposition. Think of the calcium as a scar. Whilst the calcium is inert and not dangerous, the amount of calcium correlates with the total burden of coronary atheroma and therefore, with the risk of future coronary events.
How it’s done
No IV contrast is required. The scan time is only a few seconds with set up time of less than five minutes. There is minimal radiation exposure. The amount and density of calcium in the coronary artery walls is measured to derive a calcium score. Importantly, this test only quantifies coronary calcium and does not define any soft plaque or coronary artery narrowing.
Who to scan?
In the asymptomatic, a calcium score of zero implies a very low risk in the short to medium term and generally provides reassurance which is additive to standard risk scores. The risk profile of two thirds of patients will be reclassified from intermediate to low or high risk, and guide the aggressiveness of risk factor management when compared to current risk scores. Up to 15% of intermediate risk patients have non-calcified atheroma despite a zero score which may provide false reassurance.
In symptomatic individuals a calcium score alone is not indicated. A CT coronary angiogram (CTCA) is recommended as it will visualise non-calcified soft plaque or coronary artery stenosis. Many practices include a calcium score with a CTCA.
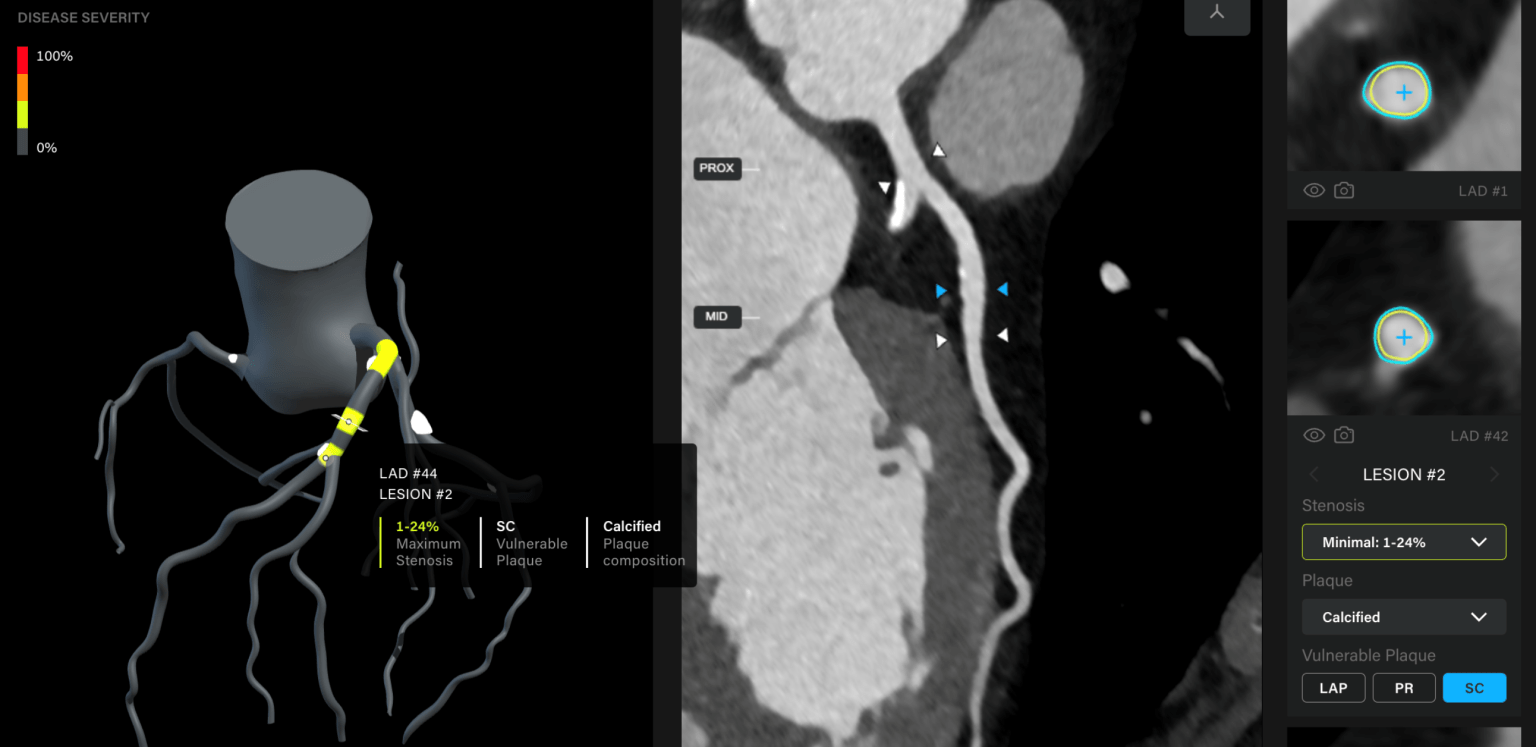
CT Coronary Angiogram (CTCA):
CTCA is a diagnostic test which allows visualisation of the coronary artery lumen to rule out stenosis and also define the presence of vulnerable, soft (non-calcified) atheroma. The amount of plaque seen is also a strong risk predictor. The more plaque seen, the higher the risk.
How it’s done
After sublingual GTN to dilate the coronary arteries, and IV contrast, ECG guided CT images are acquired. The engineering of specifically designed cardiac imaging CT scanners is quite extraordinary. To minimise blur due to cardiac motion, scans need to be super-fast (the two tonne CT scanner at Envision spins once every 230msec!) Not all CT scanners are the same (a Toyota is not a Ferrari) with significant differences in spatial and temporal (blur) resolution. It’s important to do your homework before referring.
Who to scan?
For chest pain that is indeterminate (“equivocal chest discomfort”) in a patient who is intermediate risk, then the investigation of choice is a CTCA. A normal CTCA effectively rules out coronary artery disease as a cause of the symptoms (specificity ~ 99.9%) and in 8% of cases, defines another cause for the symptoms e.g. lung cancer, pulmonary embolus, hiatus hernia, pneumonia, etc.
In Australia, the Federal government provides a Medicare rebate for some CTCAs referred by a Specialist. As always, cost is a hall of mirrors and depends on scanner quality, experience of imagers and many other factors. There is no rebate yet for a calcium score.